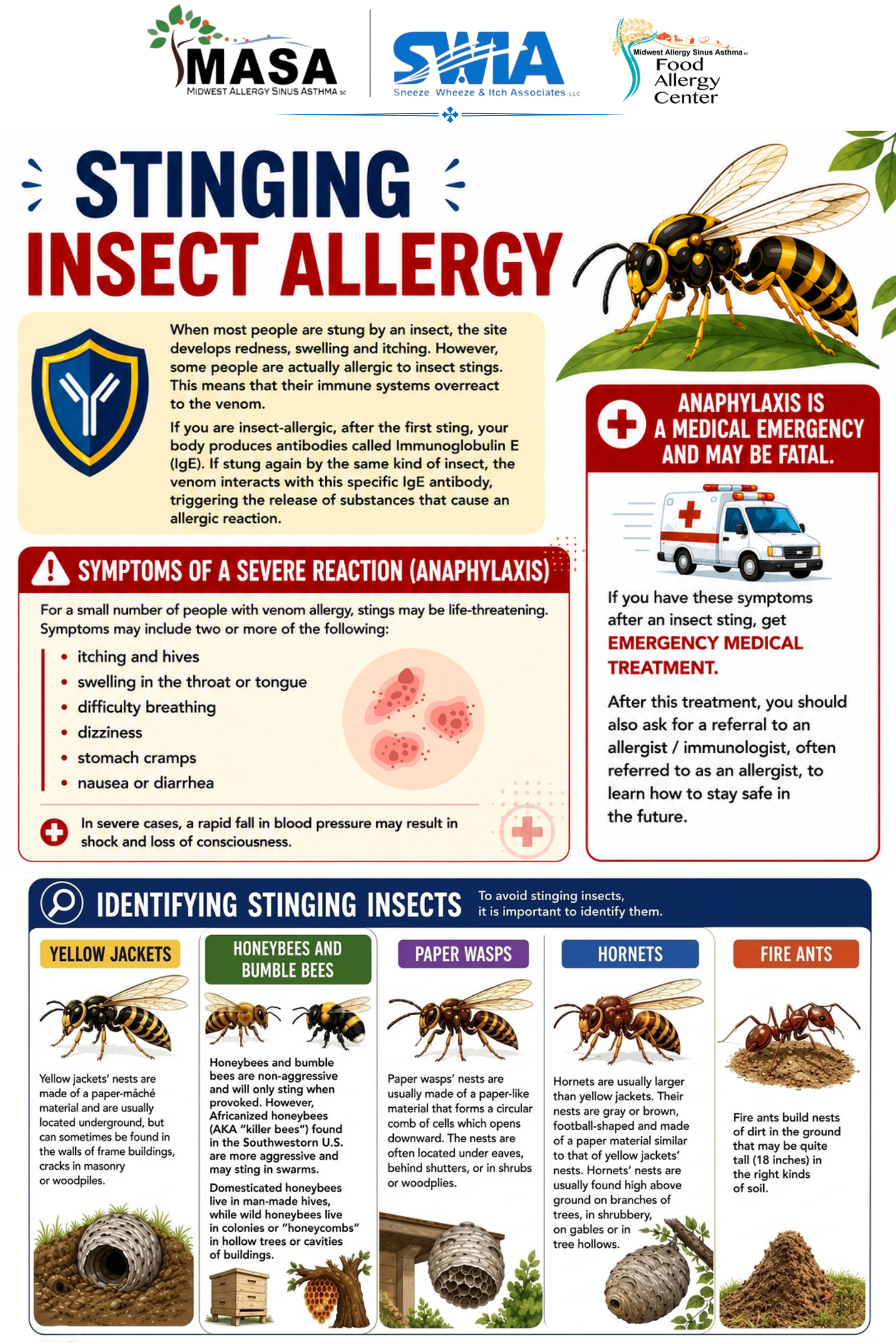

What Are Stinging Insects?
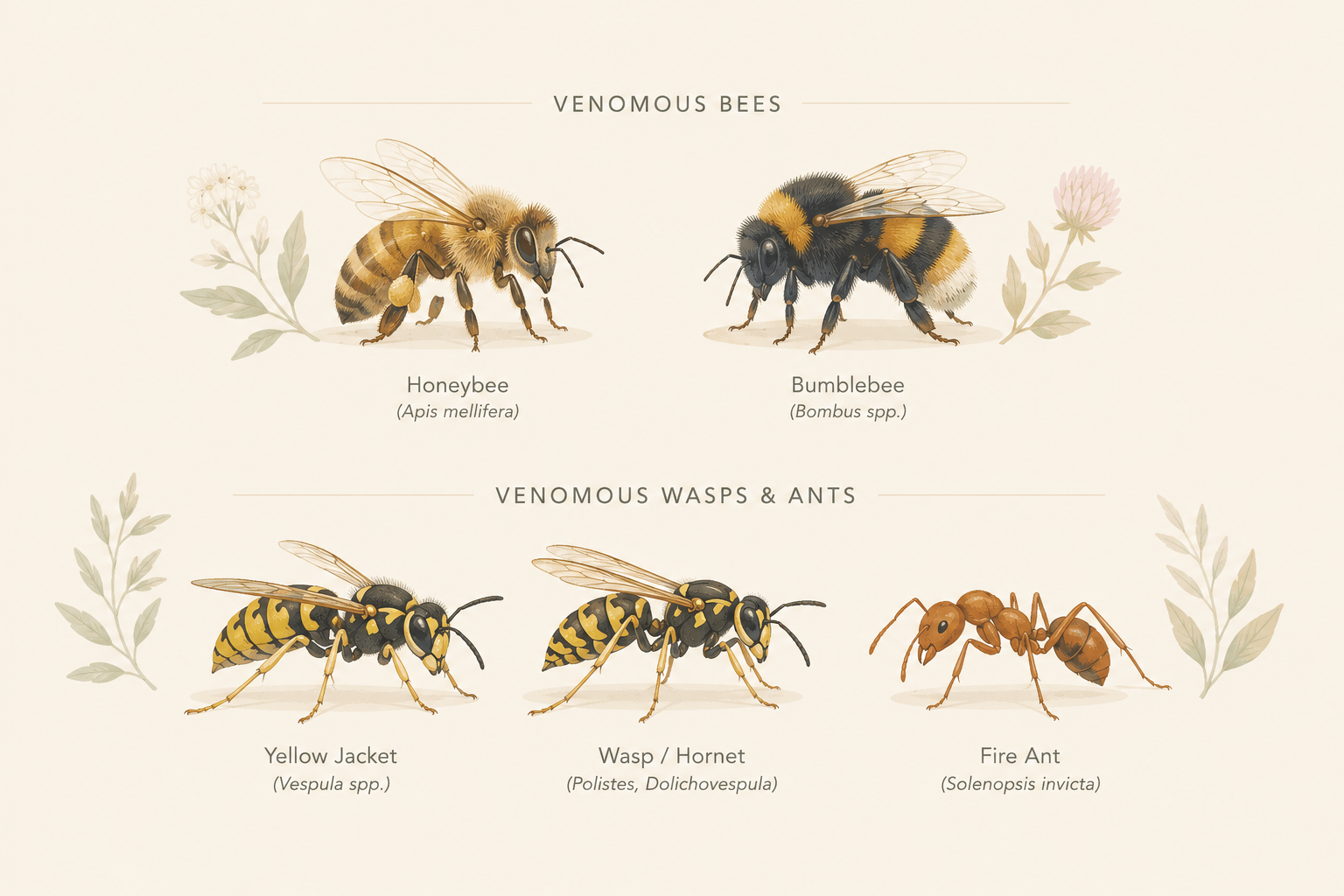
Stinging insects are members of the order Hymenoptera. In the United States, the most medically important stinging insects include:
Venomous Bees
|
Venomous Wasps & Ants
|
What Is Insect Venom?
Insect venom is a complex mixture of proteins, enzymes, and chemicals injected through the stinger. Key components include:
- Phospholipase A2 and hyaluronidase — enzymes that break down cell membranes and connective tissue, triggering inflammation
- Melittin (in bee venom) — the primary pain-producing agent
- Antigen 5 (in vespid venoms) — a major allergen recognized by the immune system
- Histamine and vasoactive amines — cause immediate local swelling, redness, and pain
In allergic individuals, the immune system mistakenly identifies these venom proteins as threats and produces IgE antibodies against them. A subsequent sting triggers mast cell activation, releasing histamine and other chemicals — this can cause a severe allergic reaction called anaphylaxis.
How Is Stinging Insect Allergy Diagnosed?
Diagnosing stinging insect allergy involves a careful history and one or more of the following tests:
| Serum-Specific IgE Blood Testing: Measures venom-specific IgE antibodies in your blood. This test is most accurate when performed no sooner than 4 weeks after a sting event. Testing too soon after a sting may produce a false-negative result because antibodies need time to recover to detectable levels (a phenomenon called “immune exhaustion”).
Skin Testing (Intradermal): Small amounts of individual venom extracts are injected just beneath the skin. This highly sensitive test is typically performed after blood testing or when blood test results remain inconclusive. Your allergist will determine the appropriate timing. Clinical History: Details of your reaction — symptoms, timing, and which insect stung you — are critical to guiding both testing and treatment decisions. |
What Is Venom Immunotherapy (VIT)?
Venom Immunotherapy (VIT), also called venom allergy shots, is a proven treatment that desensitizes your immune system to insect venom. It is highly effective and can reduce the risk of a future anaphylactic reaction from over 60% down to 1–3%.
| Build-Up Phase | Weekly injections of gradually increasing venom doses over approximately 8–28 weeks until the maintenance dose is reached. |
| Maintenance Phase | Monthly injections at the maintenance dose. Most patients remain on maintenance therapy for a minimum of 3–5 years. Some high-risk patients (e.g., those with mastocytosis or prior severe reactions) may require indefinite therapy. |
| Multiple Venoms | You may be receiving injections with more than one venom if testing shows allergy to multiple insect species. Each venom is specifically selected based on your individual allergy test results. |
The Evidence: How Well Does VIT Work?
Decades of clinical research support VIT as one of the most effective treatments in allergy medicine:
| Golden et al. (NEJM, 2004): VIT reduces the risk of systemic allergic reaction upon re-sting from approximately 60% to less than 5%.
Müller et al. (Allergy, 2008): Long-term follow-up studies show that protection persists years after completing a full course of VIT. Ruëff et al. (Allergy, 2009): Patients with higher baseline risk (history of severe anaphylaxis, elevated baseline tryptase) benefit substantially from sustained VIT. EAACI Guidelines (Allergo Journal, 2015): International consensus recommends VIT for adults with systemic reactions and positive venom-specific IgE as the standard of care. |
Frequently Asked Questions (FAQ)
| Question | Answer |
| Does VIT hurt? | Injections cause a small pinch and mild local swelling at the injection site. Significant reactions are uncommon but monitored for during your 20–30 minute wait period after each shot. |
| How long will I need the shots? | Most patients receive VIT for 3–5 years. After completing therapy, protection is long-lasting. Your allergist will reassess your risk level and determine your recommended duration. |
| Can I stop early if I feel fine? | No. Stopping early significantly increases the chance that you will lose your protection. Always discuss discontinuation with your allergist before making any changes. |
| Why am I getting more than one venom? | Testing may show allergy to multiple insect species. Each venom contains unique proteins, so each requires its own desensitization. This is normal and expected. |
| What if I get stung while on VIT? | Contact our office. Early in the build-up phase protection is not yet complete. You should always carry your epinephrine auto-injector and use it if systemic symptoms develop. |
| Do I need VIT if my reaction was only local swelling? | Large local reactions (swelling beyond the sting site) do NOT typically require VIT. Your allergist will help determine if you are a candidate. |
Important Medication Considerations
| ⚠ Beta-Blockers & ACE Inhibitors: Special Precautions
Certain blood pressure medications can interfere with your ability to respond to epinephrine and worsen the severity of anaphylaxis: Beta-blockers (e.g., metoprolol, atenolol, propranolol) block the receptors that epinephrine acts on, making treatment of anaphylaxis more difficult. ACE inhibitors (e.g., lisinopril, enalapril) are associated with increased risk of severe reactions. If you have had a severe anaphylactic reaction to stinging insects or are at high ongoing risk, please discuss these medications with both your allergist and prescribing physician. Switching to alternative agents may be recommended. |
Mast Cell Disorders & Stinging Insect Anaphylaxis
Some patients who experience stinging insect anaphylaxis — particularly those with cardiovascular symptoms such as low blood pressure, dizziness, loss of consciousness, or rapid heart rate — may have an underlying mast cell disorder such as:
- Systemic Mastocytosis (SM) — abnormal accumulation of mast cells in bone marrow and/or other organs
- Mast Cell Activation Syndrome (MCAS) — episodes of inappropriate mast cell activation without significant accumulation
- Clonal Mast Cell Disease — a spectrum of disorders involving KIT D816V mutation
| Why This Matters: Mast cell disorders significantly elevate the risk of severe and fatal reactions to stinging insects. Early identification leads to appropriate risk management, consideration of indefinite VIT, and targeted treatment.
Serum Tryptase: A baseline serum tryptase level is a key screening test. Elevated tryptase (particularly >11.4 ng/mL, or a value >1 + 2× baseline) may indicate clonal mast cell disease. When to Screen: Screening is recommended for patients who experienced cardiovascular symptoms (low blood pressure, syncope, or near-syncope) during a stinging insect anaphylaxis event, even if reaction severity seemed moderate overall. |
How to Avoid Stinging Insects: Environmental Tips
Outdoors
|
Home & Vehicle
|
Always Carry Your Epinephrine Auto-Injector
| ⚠ This Is Non-Negotiable
Even while receiving Venom Immunotherapy, you must carry two epinephrine auto-injectors (e.g., EpiPen®, Auvi-Q®) or Neffy® Nasal ephinrine at ALL times until your allergist advises otherwise. Epinephrine is the FIRST and ONLY first-line treatment for anaphylaxis. Antihistamines and steroids are not substitutes and do not reverse anaphylaxis. Use epinephrine immediately if you develop any of the following after a sting: hives/flushing beyond the sting site, throat tightness, difficulty breathing, dizziness, low blood pressure, or loss of consciousness. After using epinephrine: CALL 9-1-1 IMMEDIATELY and go to the nearest emergency room. A second dose may be needed. Check your auto-injector expiration date every 6 months and replace promptly when expired. |
Contact Midwest Allergy Sinus Asthma, SC
| Questions or Concerns?
📞 (309) 452-0995 or (217) 717-4404 🌐 www.asthma2.com ✉ Contact us through our patient portal |
After-Hours / Emergency
If you experience a severe allergic reaction: 1. Use your epinephrine auto-injector 2. Call 9-1-1 immediately 3. Go to nearest emergency room |
This educational handout is intended for informational purposes only and does not replace individualized medical advice from your allergist.