This clinical guide provides a technical overview of mast cell disorders, categorizing them into three primary classifications: clonal overgrowth, inappropriate activation, and inherited high-tryptase states.
Mast Cell Disorders: Clinical Classification & Diagnostic Framework
Mast cell disorders are complex multi-system conditions. To provide effective clinical management, it is essential to distinguish between mast cell overgrowth (clonal disease), inappropriate activation (MCAS), and inherited genetic states such as Hereditary Alpha-Tryptasemia or HAT.
1. Mastocytosis: Clonal Overgrowth
Mastocytosis is defined by an abnormal proliferation of mast cells, frequently associated with KIT mutations (specifically KIT D816V in systemic cases).
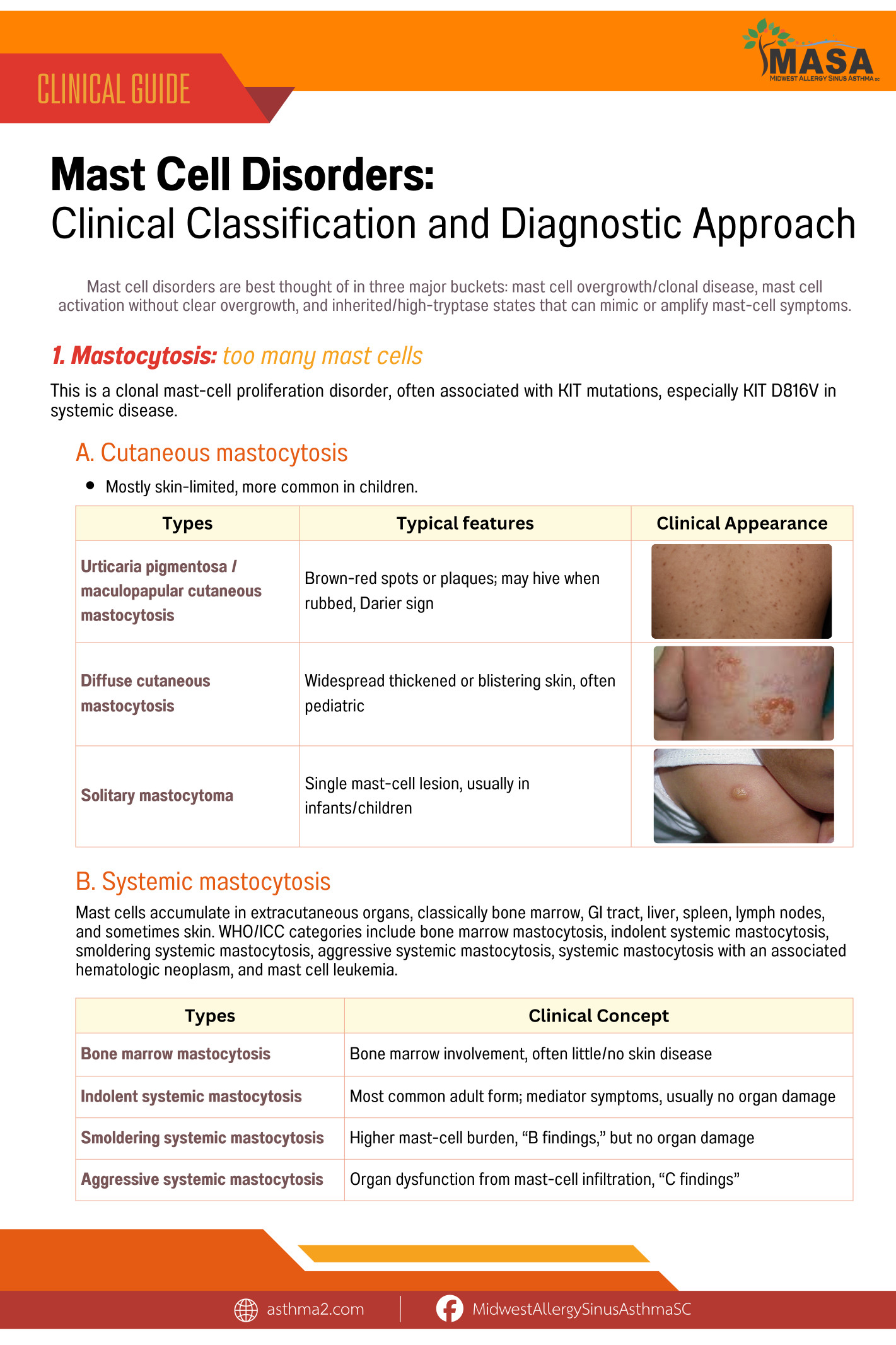
A. Cutaneous Mastocytosis
Commonly seen in pediatric patients, this form is largely limited to the skin.
-
Urticaria pigmentosa: Characterized by brown-red spots or plaques that hive when rubbed (Darier sign).
-
Diffuse cutaneous mastocytosis: Widespread skin thickening or blistering.
-
Solitary mastocytoma: A single mast-cell lesion, typical in infants.
B. Systemic Mastocytosis (SM)
In SM, mast cells accumulate in extracutaneous organs such as bone marrow, the GI tract, liver, and spleen.
-
Non-Advanced SM: Includes Indolent SM (most common in adults) and Smoldering SM.
-
Advanced SM: Includes Aggressive SM (organ dysfunction), SM-AHN (associated with other blood disorders), and Mast Cell Leukemia.
2. Mast Cell Activation Syndrome (MCAS)
MCAS occurs when mast cells release mediators inappropriately despite a normal cell count. Symptoms resemble recurrent anaphylaxis, affecting two or more organ systems (e.g., flushing, angioedema, hypotension, tachycardia, and brain fog).
Diagnostic Criteria:
-
Systemic Symptoms: Recurrent episodes involving multiple organ systems.
-
Objective Mediator Rise: A rise in tryptase during an event using the “20% + 2” rule over baseline.
-
Clinical Response: Improvement when treated with mast-cell-directed therapy (H1/H2 blockers, leukotriene modifiers, cromolyn, etc.).
MCAS Classifications:
-
Primary/Clonal: Evidence of KIT mutation or aberrant markers (CD25/CD2/CD30).
-
Secondary: Activation due to an underlying condition (allergy, venom, autoimmune disease).
-
Idiopathic: Criteria met, but no clonal or secondary cause is identified.
3. Hereditary Alpha-Tryptasemia (HAT)
HAT is an inherited condition caused by increased copy numbers of the TPSAB1 gene. It often leads to a chronically elevated baseline tryptase (>8 ng/mL). While not mastocytosis or MCAS itself, it can coexist with and amplify the symptoms of both, increasing the tendency for anaphylaxis, GI symptoms, and hypermobility.
4. Mast-Cell-Mediated Allergic Diseases
Though often categorized as general allergies, several conditions are primarily driven by mast cell activity. In these cases, the mast cell plays a specific role in the disease pathology:
-
IgE-Mediated Food Allergy: Driven by mast-cell degranulation immediately following allergen exposure.
-
Venom Allergy: Can produce severe anaphylaxis. This is a critical area of concern, as a pre-existing mastocytosis condition significantly increases the risk of a life-threatening venom reaction.
-
Drug Allergy: Involves mast-cell activation through both IgE and non-IgE pathways.
-
Chronic Spontaneous Urticaria: Primarily caused by the activation of mast cells and basophils within the skin tissue.
-
Anaphylaxis and Idiopathic Anaphylaxis: Defined by a systemic release of mast-cell mediators throughout the body.
5. Monoclonal Mast Cell Activation Syndrome (mMCAS)
Monoclonal Mast Cell Activation Syndrome represents a vital “in-between” diagnosis. In these cases, a patient exhibits clonal mast-cell markers—such as the KIT D816V mutation or aberrant CD25/CD2/CD30 expression—yet they do not meet the full diagnostic criteria for systemic mastocytosis. These patients typically present with high-risk symptoms, including recurrent anaphylaxis, hypotension, flushing, or severe reactions to insect venom.
6. Rare Localized Mast-Cell Tumors
In rare instances, mast cells can cluster to form localized tumors. These are classified based on their location and severity:
-
Mastocytoma: These are usually cutaneous (skin-based) and are most frequently diagnosed in pediatric patients.
-
Extracutaneous Mastocytoma: A rare version of a localized mast cell mass that occurs outside of the skin.
-
Mast Cell Sarcoma: An extremely rare and aggressive malignant form of a mast-cell tumor.
Practical Diagnostic Sorting: What Clinical Findings Mean
Effective diagnosis requires “sorting” clinical findings to determine the most likely underlying pathology.
If a patient presents with a persistently elevated baseline tryptase, especially levels above 20, clinicians should investigate Systemic Mastocytosis, Hereditary Alpha-Tryptasemia (HαT), renal disease, or myeloid neoplasms. If the baseline tryptase is above 8 ng/mL and accompanied by a relevant family history, testing for Hereditary Alpha-Tryptasemia is indicated.
When symptoms include episodic anaphylaxis accompanied by a rise in tryptase, the primary considerations are MCAS or a standard anaphylaxis disorder. A positive KIT D816V blood test is a strong indicator of clonal mast-cell disease and warrants a bone marrow evaluation.
Physical examinations also provide key clues. Skin lesions exhibiting the Darier sign (hiving when rubbed) suggest cutaneous or systemic mastocytosis. Finally, more severe findings such as organ damage, cytopenias, hepatosplenomegaly, or pathologic fractures require an immediate and thorough evaluation for Advanced Systemic Mastocytosis.
For Clinicians: Partner with MASA
Navigating the complexities of mast cell disorders requires a nuanced, multidisciplinary approach. At Midwest Allergy Sinus Respiratory (MASA), our team, led by Dr. Dareen Siri, specialize in the advanced diagnostic testing and long-term management of Mastocytosis, MCAS, and HAT.
If you have a patient presenting with multisystem symptoms or elevated tryptase, we invite you to collaborate with us. We are committed to working alongside primary care providers and specialists to provide comprehensive, evidence-based care.
Contact us for referrals or clinical consultations:
-
Phone: 309-452-0995 (Normal, Peoria satellite) | 217-717-4404 (Springfield, Carlinville and Jacksonville satellites)
-
Facebook: MidwestAllergySinusAsthmaSC