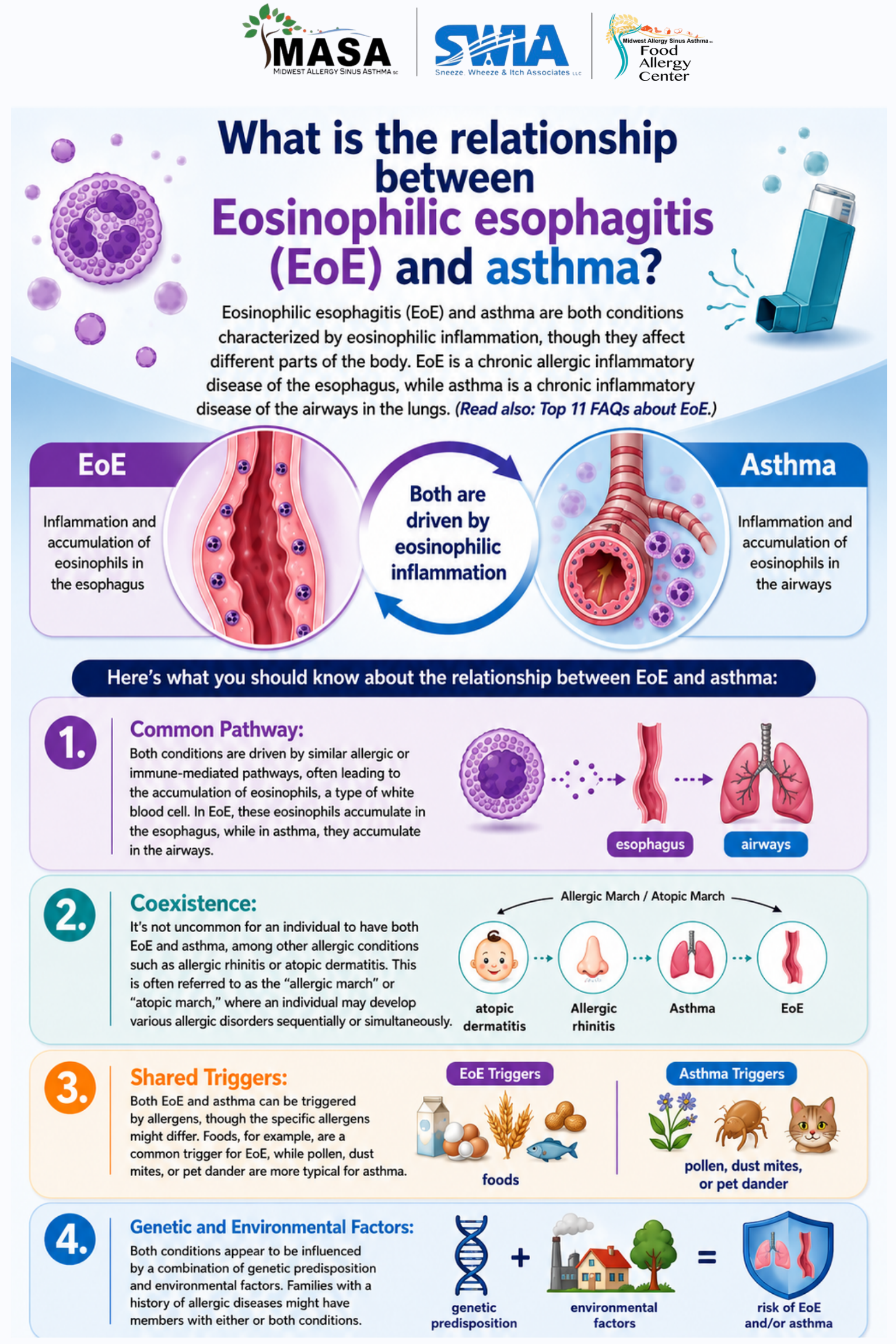
Eosinophilic esophagitis (EoE) and asthma are both conditions characterized by eosinophilic inflammation, though they affect different parts of the body. EoE is a chronic allergic inflammatory disease of the esophagus, while asthma is a chronic inflammatory disease of the airways in the lungs. (Read also: Top 11 FAQs about EoE.)
Here’s what you should know about the relationship between EoE and asthma:
- Common Pathway: Both conditions are driven by similar allergic or immune-mediated pathways, often leading to the accumulation of eosinophils, a type of white blood cell. In EoE, these eosinophils accumulate in the esophagus, while in asthma, they accumulate in the airways.
- Coexistence: It’s not uncommon for an individual to have both EoE and asthma, among other allergic conditions such as allergic rhinitis or atopic dermatitis. This is often referred to as the “allergic march” or “atopic march,” where an individual may develop various allergic disorders sequentially or simultaneously.
- Shared Triggers: Both EoE and asthma can be triggered by allergens, though the specific allergens might differ. Foods, for example, are a common trigger for EoE, while pollen, dust mites, or pet dander are more typical for asthma.
- Genetic and Environmental Factors: Both conditions appear to be influenced by a combination of genetic predisposition and environmental factors. Families with a history of allergic diseases might have members with either or both conditions.
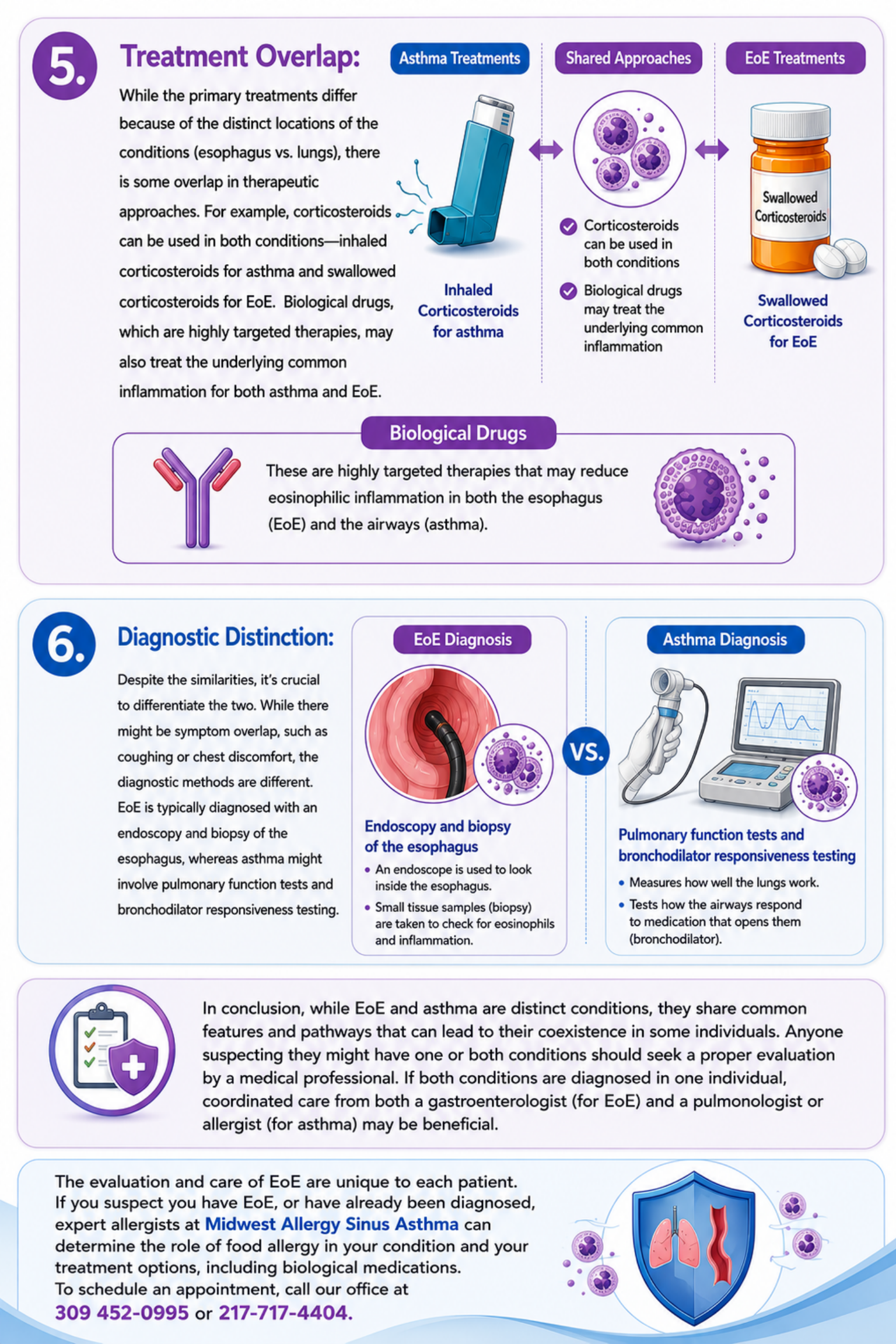
- Treatment Overlap: While the primary treatments differ because of the distinct locations of the conditions (esophagus vs. lungs), there is some overlap in therapeutic approaches. For example, corticosteroids can be used in both conditions—inhaled corticosteroids for asthma and swallowed corticosteroids for EoE. Biological drugs, which are highly targeted therapies, may also treat the underlying common inflammation for both asthma and EoE.
- Diagnostic Distinction: Despite the similarities, it’s crucial to differentiate the two. While there might be symptom overlap, such as coughing or chest discomfort, the diagnostic methods are different. EoE is typically diagnosed with an endoscopy and biopsy of the esophagus, whereas asthma might involve pulmonary function tests and bronchodilator responsiveness testing.
In conclusion, while EoE and asthma are distinct conditions, they share common features and pathways that can lead to their coexistence in some individuals. Anyone suspecting they might have one or both conditions should seek a proper evaluation by a medical professional. If both conditions are diagnosed in one individual, coordinated care from both a gastroenterologist (for EoE) and a pulmonologist or allergist (for asthma) may be beneficial.
The evaluation and care of EoE are unique to each patient. If you suspect you have EoE, or have already been diagnosed, expert allergists at Midwest Allergy Sinus Asthma can determine the role of food allergy in your condition and your treatment options, including biological medications. To schedule an appointment, call our office at 309 452-0995 or 217-717-4404.
We always have an on-going paid clinical trials for interested patients. Please visit our clinical trials page to see if you are eligible and would like to participate in the program to get close care from your provider and benefit research.